Table of Contents
Cubital Fossa Overview
The cubital fossa (Latin for “elbow”) is a triangular hollow on the front of the elbow. (It is similar to the lower limb’s popliteal fossa, which is located on the back of the knee.)
Dissection
Identify the structures that can be found in the roof of a shallow cubital fossa on the front of the elbow. Separate the lateral and medial boundaries created by the brachioradialis and pronator teres muscles, respectively.
Organize the contents:
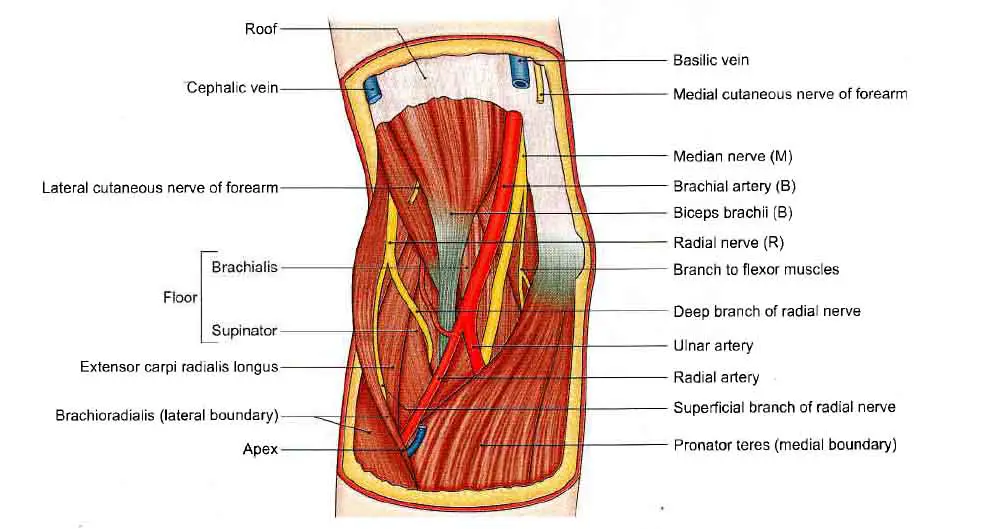
- The median nerve on the medial side of the brachial artery.
- The terminal part of the brachial artery bifurcating into radial and ulnar arteries.
- The biceps brachii muscle’s tendon between the brachial artery and radial nerve.
- The radial nerve on a deeper plane on the lateral side of the biceps tendon.
Recognize the brachialis and supinator muscles, which form the floor of the cubital fossa.
Boundaries
Laterally: The brachioradialis(medial border)
Medially: The pronator teres(lateral border)
Base: It is directed upwards and is defined by an imaginary line connecting the front of two humeral epicondyles.
Apex: It is formed by the meeting point of the lateral and medial boundaries and is directed downwards.
Roof
The roof is formed by;
- Skin
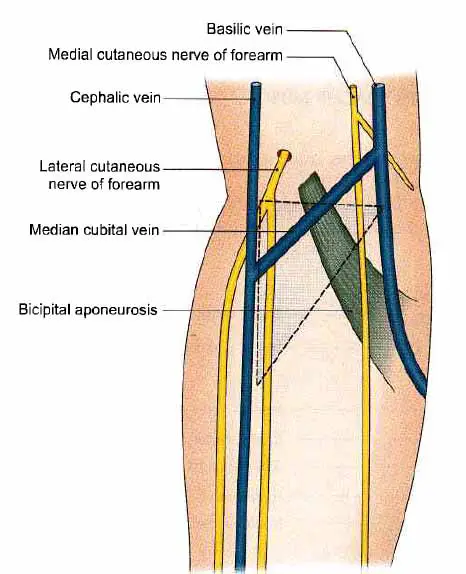
- Superficial fascia: The median cubital vein connects the cephalic and basilic veins in the superficial fascia. The lateral cutaneous nerve of the forearm runs parallel to the cephalic vein, while the medial cutaneous nerve of the forearm runs parallel to the basilic vein.
- Deep fascia.
- Bicipital aponeurosis.
Floor
The floor is formed by;
- Brachialis
- Supinator surrounding the upper part of the radius.
Read Cephalic Vein
Contents
The fossa is very narrow. After retracting the boundaries, the mentioned contents are revealed. The contents are as follows, from medial to lateral.
- The Median Nerve: It passes between the two heads of pronator teres and gives branches to flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and leaves the fossa.
- The fossa contains the brachial artery’s end and the beginnings of the radial and ulnar arteries.
Read The Radial Artery
The radial artery is narrower and superficial than the ulnar artery. It forms the radial recurrent branch. The ulnar artery branches are deep to both heads of the pronator teres and pass downwards and medially, separated from the median nerve by the pronator teres’ deep head.
The anterior ulnar recurrent, posterior ulnar recurrent, and common interosseous branches arise from the ulnar artery.
The anterior and posterior interosseous arteries split the common interosseous branch, and the latter gives off the interosseous recurrent branch.
- The biceps brachii tendon and the bicipital aponeurosis.
- The radial nerve (along with the radial collateral artery) appears between the brachialis (medially) and the brachioradialis and extensor carpi radialis longus laterally. The radial nerve provides the three flanking muscles when running in the intermuscular gap, and just below the level of the lateral epicondyle it gives off the posterior interosseous nerve or deep branch of the radial nerve, which leaves the fossa by penetrating the supinator muscle. The remaining superficial branch continues for a short distance in front of the forearm.
Read The Ulnar Artery
Clinical Anatomy
The cubital region is important for many reasons, some these are;
- The median cubital vein is used mostly for intravenous injections.
- The brachial artery in front of the elbow is universally used to measure blood pressure.
The anatomy of the cubital fossa is helpful when dealing with fractures around the elbow, such as the supracondylar humeral fracture.
Supracondylar Fracture
Read The Basilic Vein
Cubital Tunnel Syndrome
Cubital tunnel syndrome is an ulnar nerve neuropathy that causes numbness and shooting pain along the medial aspect of the forearm, as well as the medial half of the fourth and fifth digits. It is caused by ulnar nerve compression in the elbow area.
Anatomy of Ulnar nerve
The C8 and T1 nerve roots connect to form the brachial plexus medial cord. It is a branch of the medial cord. The ulnar nerve then follows the brachial artery down the arm to the elbow joint. The nerve enters the posterior compartment at the midpoint of the arm by penetrating the intermuscular septum (arcade of Struthers). It then travels along the triceps’ medial aspect to reach the cubital tunnel. The ulnar nerve passes between the olecranon and the medial epicondyle, underneath the Osborne ligament, at this stage. The nerve leaves the cubital tunnel and enters the forearm through the aponeurotic head of the flexor carpi ulnaris. Because of its position and anatomy, the ulnar nerve is most likely to be compressed in the cubital tunnel area. However, the nerve may be squeezed at the arcade of Struthers or by the aponeurotic head of the flexor carpi ulnaris, leading to ulnar neuropathy symptoms. The ulnar nerve is found in the forearm’s medial side, the palm’s ulnar side, the little finger, and the ulnar half of the ring finger. It gives motor branches to the flexor carpi ulnaris, the flexor profundus of the little and ring fingers, the hypothenar muscles, the adductor pollicis brevis, all of the interossei, and the third and fourth lumbricals. It is worth noting that the ulnar nerve does not have any motor or sensory branches above the elbow.
Common Causes
Pressure: Symptoms are often caused by pressure on the ulnar nerve. Since the ulnar nerve is very superficial at the point of the medial epicondyle, people who unintentionally hit their elbow on a hard surface can experience shooting pain and electric shock in the forearm.
Stretching: Related symptoms may be caused by stretching the ulnar nerve. Below the medial epicondyle is the ulnar nerve. Because of this anatomical location, the ulnar nerve is extended during elbow flexion. Repetitive elbow flexion and extension will aggravate and irritate the ulnar nerve. Some people sleep with their elbows bent, which can stretch the ulnar nerve for a prolonged period of time during sleep and is a known cause of ulnar nerve discomfort.
Injuries: Injuries to the elbow joint (fractures, dislocations, swelling, effusions) may result in anatomical damage that causes symptoms due to ulnar nerve compression/irritation.
Cubital tunnel syndrome’s precise pathophysiology is unclear. There have been some connection with smoking. Males are more likely to be affected than females, and the left side is more often affected.
Treatment
When deciding on treatment choices, pathological results should be carefully evaluated. Patients will also benefit from non-surgical interventions; thus, clinicians should assess and establish an end goal for care with the patient before agreeing on a treatment path.
Non-Surgical
- If the symptoms are caused solely by mechanical causes, such as leaning over a desk at work with weight on the elbows or sleeping with bent elbows, then changing the postures that cause ulnar neuropathy may be the mainstay of treatment.
- A study in Italy showed up on 24 patients who had refused surgery after their initial diagnosis in an Italian study. During their follow-up visits, about half of these patients showed improvement in their symptoms. Their subsequent nerve conduction tests have revealed an increase, adding to the evidence that patients with moderate symptoms can be treated without surgery.
- Splinting at night to hold the elbows straight has been proposed as an initial management option in patients with moderate symptoms in published articles.
- Simple analgesics, such as NSAIDs, can also alleviate pain.
Surgical
Patients with extreme signs and symptoms, such as interossei atrophy and handgrip strength loss, do not improve with conservative care. Furthermore, patients who have failed conservative care for 6 months will need surgical intervention to alleviate their symptoms. The nerve is decompressed in the entire cubital tunnel during surgery. Some surgeons prefer to relieve pressure in the cubital tunnel area, while others prefer free ulnar nerve mobilization.
Various surgical treatment approaches have been debated and implemented. Any of the well-accepted surgical procedures for cubital tunnel syndrome care are as follows:
- Decompression in-situ;
- Endoscopic decompression
- Decompression accompanied by subcutaneous, intramuscular, or submuscular transposition, and
- Medial epicondylectomy with in-situ decompression
In terms of clinical results, studies have found little advantage of one over the other.
Read The Brachial Pulse
Complications
- After surgical decompression, one out of every eight patients may experience a recurrence of their symptoms. The most common reason for revision surgery has been insufficient decompression.
- It is possible that recovery will be slow and incomplete.
- Symptoms can worsen before improving.
- Injury to the forearm’s medial antebrachial cutaneous nerve is a common complication of cubital tunnel release and may result in a painful neuroma.
Few Last Words about Cubital Fossa
The cubital fossa (also known as the antecubital fossa) (plural: fossae) is an inverted triangular area that connects the arm to the forearm. It is found just forward of the elbow joint.
Last Updated on February 23, 2022 by Learn From Doctor Team




