Table of Contents
Radial Artery Beginning, Course, and Termination
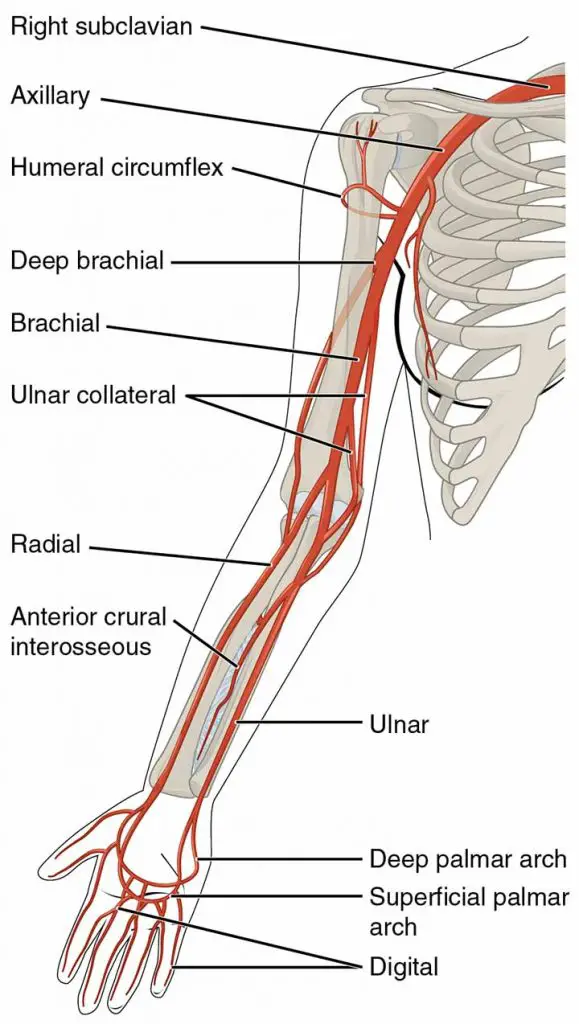
The radial artery is the brachial artery’s smaller terminal branch in the cubital fossa. It has a lateral convexity and runs downward to the elbow. It exits the forearm by turning backward and entering the anatomical snuff box. It is very shallow in its entire course as compared to the ulnar artery. Its distribution in the hand is discussed further below.
Relation
Anteriorly
In the upper half, it is overlapping by the brachioradialis, but in the lower half, it is only covered by skin, superficial and deep fasciae.
Posteriorly
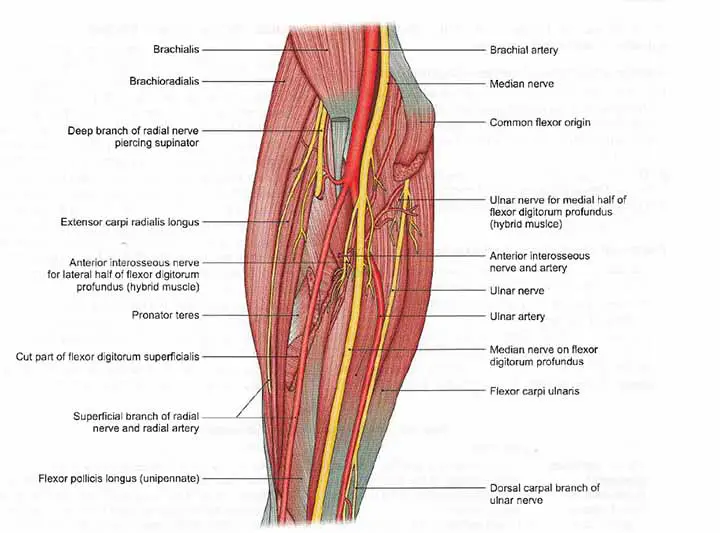
It is related to the muscles attached to the anterior surface of the radius, these are;
- Biceps brachii,
- Flexor pollicis longus,
- Flexor digitorum superficialis
- Pronator quadratus.
Read Ulnar Artery | Hand Specialist | Hand Surgeon
Medially
It is related to the pronator teres in the upper one-third of its route and the flexor carpi radialis tendon in the lower two-thirds.
Laterally
Brachioradialis in and radial nerve throughout the middle one-third
The radial artery is accompanied by venae comitantes.
Branches(in the forearm)
- The radial recurrent artery: It begins just below the elbow, travels deep to the brachioradialis, and terminates by anastomosing with the radial collateral artery (anterior branch of the profunda brachii artery) in front of the lateral epicondyle of the humerus.
- Muscular Branches: The lateral muscles of the forearm are given muscular branches.
- The palmar carpal branch: The palmar carpal branch develops near the lower border of the pronator quadratus, runs medially deep to the flexor tendons, and ends with a cruciform anastomosis with the palmar carpal branch of the ulnar artery, in front of the center of the recurrent branch of the deep palmar arch. The palmar carpal arch is responsible for supplying bones and joints at the wrist.
- The dorsal carpal branch: It connects to a branch of the ulnar artery to form the dorsal carpal arch.
- The superficial palmar branch: The superficial palmar branch develops just before the radial artery exits the forearm by winding backward. The branch runs through the thenar muscles before connecting to the terminal part of the ulnar artery to complete the superficial palmar arch.
Read The Allen’s Test
Read Cephalic Vein
Surface Marking
On Forearm
The radial artery is marked on the forearm by joining the following points;
- A point in front of the elbow at the level of the radius neck medial to the biceps brachii tendon.
- The second point at the wrist where the radial pulse is usually felt is between the anterior border of the radius laterally and the tendon of the flexor carpi radialis medially.
It follows a curved path with a gentle convexity on the lateral side.
On Hand
The radial artery is marked on the hand by joining the following points;
- A point on the wrist between the anterior border of the radius and the flexor carpi radialis tendon.
- A second point just below the tip of the radius’s styloid process.
- The third point is located near the proximal end of the first intermetacarpal space.
The artery runs obliquely downwards and backward in this section, deep to the tendons of the abductor pollicis longus and extensor pollicis brevis, and superficial to the lateral ligament of the wrist joint. As a result, it travels through the anatomical snuff box to the proximal end of the first intermetacarpal space.
Read The Axillary Artery
Clinical Anatomy
Radial Artery Laceration
When comparing operative and nonoperative approaches to forearm lacerations, it was discovered that penetrating damage to the forearm requires treatment for limb-threatening ischemia. In this case, surgical management is needed to restore blood flow. However, due to the extensive anastomotic connections between the radial and ulnar arteries in the hand, isolated laceration of either artery is not usually fatal. It is safe and permissible to ligate a distal forearm artery in the presence of weak hemostasis as long as sufficient perfusion occurs at the palmar arch. Surgical repair is needed in the case of complex lacerations affecting both the radial and ulnar arteries. It has been known that functional impairment is caused by the severity of concomitant nerve damage rather than arterial injury.
Arterial Grafts
The left internal mammary artery (LIMA), also known as the internal thoracic artery, has been the preferred conduit for the LAD.
Long-term patency rates of more than 98 percent have been recorded since the mid-1980s, with increased long-term survival and fewer reoperations. Since LIMA–LAD anastomosis prevents the late complication of vein graft atherosclerosis, researchers have been particularly interested in the use of bilateral internal mammary artery (BIMA) grafts. However, there is continuing concern about its appropriateness in some patient subgroups, such as obese diabetics, who tend to have a higher risk of sternal wound complications.
The use of the radial artery as a secondary or alternative arterial bypass graft has recently seen a resurgence. To some degree, this has been motivated by the emerging idea of complete arterial revascularisation and the assumption that this would further increase the long-term outcomes of coronary surgery. Several randomized controlled trials have shown excellent patency rates at 1 and 5 years. When evaluating a patient for a radial artery harvest, Allen’s test should be performed. The gastroepiploic artery and the inferior epigastric artery are two alternative arterial bypass grafts.
Arteriovenous (AV) Fistulas
The radial artery has long been used to create arteriovenous fistulas for dialysis. Jennings et al. indicated in a paper that the proximal radial artery was an excellent site for low-risk dialysis-related steal syndrome. Although it has been suggested that AV fistulas be created as far distal in the upper extremity as possible, Wu et al. reported low to moderate primary failure of proximal radial artery arteriovenous fistulas (PEAAVF) when chosen as the primary site of PRAAVF formation; the primary failure rate reached 12.3 percent.
The Radial Pulse
A typical place for medical professionals to document a patient’s pulse is palpation for the radial artery proximal to the wrist crease and immediately lateral to the tendon of the flexor carpi radials muscle. It can also be felt in the anatomical snuffbox when it reaches the lateral side of the elbow. The snuffbox’s medial aspect is the tendon of the extensor pollicis brevis muscle. The tendons of the extensor pollicis longus and abductor pollicis longus muscles form the lateral aspects.

Read The Brachial Pulse
Few Last Words
The radial artery is mostly used to record the pulse rate from the ancient time of civilization. It has other clinical importance also. Nowadays it’s being used for Coronary Artery Bypass Grafting.
Read The Index Finger
Last Updated on February 23, 2022 by Learn From Doctor Team




