Table of Contents
Cephalic Vein Beginning, Course, Termination
The cephalic vein is the upper limb’s preaxial vein (such as; the great saphenous vein of the lower limb). It starts at the lateral end of the dorsal venous arch of the hand.
It runs upward;
- Through the roof of the anatomical snuffbox.
- Then winds round the lateral border of the distal part of the forearm.
- Continues up to the elbow and along the lateral border of the biceps brachii.
- Penetrate the deep fascia at the lower border of the pectoralis major muscle.
- It runs in the deltopectoral groove until it reaches the infraclavicular fossa, where it pierces the clavipectoral fascia and connects to the axillary vein.
The majority of the blood at the elbow is drained into the basilic vein via the median cubital vein, and a part is also drained into the deep veins via the perforator vein.
It is followed by the forearm’s lateral cutaneous nerve and the terminal part of the radial nerve.
An accessory cephalic vein is sometimes present. It joins the cephalic vein near the elbow.
Read The Basilic Vein
Course Overview
The cephalic vein drains the hand’s dorsal venous network, which crosses the anatomical snuffbox, runs superficial to the radial styloid process, and then ascends in the forearm’s superficial fascia. The cephalic vein then connects with the basilic vein through the median cubital vein at the cubital fossa. The vein is located in the lateral part of the elbow joint crease.
The cephalic vein now continues between the brachioradialis (forearm supinator and elbow flexor) and biceps brachii (forearm supinator and elbow flexor) muscles. The vein ascends in the superficial fascia anterolateral to the biceps brachii and superficial to the lateral cutaneous nerve of the forearm, a sensory branch of the musculocutaneous nerve (ventral rami of C5-7) that innervates the muscles of the anterior compartment of the arm. The cephalic vein ascends further in a groove formed by the pectoralis major and deltoid muscles. The cephalic vein is accompanied in this area by the deltoid branch of the thoracoacromial trunk.
Read Radial Artery
Drainage Overview
It drains into the axillary vein just below the clavicle after passing through the clavipectoral fascia and the axillary artery. As the axillary vein crosses the lateral borders of the first rib, it is renamed the subclavian vein, and it joins the internal jugular vein to form the brachiocephalic vein.
Clinical Anatomy
Cephalic Vein Cut-down
Central venous access can be needed when a patient’s peripheral veins are too small or incompetent. Traditionally, this takes the form of a central line through the subclavian vein. The cephalic vein, on the other hand, has provided an option for venous access that is quicker, smoother, and does not threaten the complications of central venous access, such as pneumothorax. A cephalic vein cutdown can also be used for the percutaneous insertion of pacemaker leads into the heart and the placement of a long-term venous catheter.
Some studies proving the fact that the cephalic vein cut down technique is the safest one.
Let us check how these studies works
Background
Several techniques for inserting implantable chemotherapy ports have been developed. The cephalic vein cut down technique is regarded as a safe procedure with a high rate of success. The surgical team that installs the chemoports and the nursing team that manages them both have a learning curve.
Methods and history of patients
Both consecutive patients undergoing surgical chemoport implantation should be examined. Chemoport implantation was first attempted in the cephalic vein using a cut-down procedure, then in the subclavian or internal jugular vein using a closed Seldinger process. Surgical information was registered, and nursing personnel’s access to the chemo port was monitored. Any difficulties in accessing or using the chemoports were noted and assistance was sought.
Result
The cephalic vein cutting technique was effective in 50% of patients. It was less effective in patients who had previously received chemotherapy. The most common cause of concern when managing chemoports was a lack of blood return on entry. An algorithm for vein selection and an institutional protocol for chemoport access and use improve protection and performance.
Houseman’s friend
The staff nurse is normally in charge of collecting blood for blood tests. As a result, the superficial veins of the upper limb are the best place to reach this blood and are named the “Houseman’s Mate.” The most commonly accessed vein is the median cubital vein in the cubital fossa.
Varicose Vein
Varicose veins are enlarged, swollen, twisting veins that are mostly blue or dark purple. They occur when defective vein valves cause blood to flow in the wrong direction or pool.
Symptoms
The painless vein may show the following symptoms;
- Colored veins that are dark purple or blue
- Veins that look twisted and bulging; sometimes mimic cords on your legs.
The painful vein may show the following symptoms;
- Feeling the weight in the leg
- Pain that worsens after sitting or standing for a long period of time.
- Itching around the skin of the affected vein.
- Skin discoloration around the skin of varicose vein.
Read The Ulnar Artery
Causes
Varicose veins may be caused by faulty or damaged valves. Arteries transport blood from your heart to your tissues and veins return blood from the rest of your body to your heart, allowing blood to be recirculated. The veins in your legs must work against gravity to return blood to your core.
Lower leg muscle contractions serve as pumps, and elastic vein walls help blood return to your heart. When blood flows through your heart, tiny valves in your veins open and close to prevent blood from flowing backward. If these valves are weak or weakened, blood may flow backward and pool in the vein, stretching or twisting it.
Complications
- Venous ulcer
- Blood clot
- Abnormal bleeding
Cephalic Vein Aneurism
Cephalic vein aneurysms are uncommon malformations that can occur anywhere in the vascular system, and their history, appearance, and treatment differ based on where they occur. While many hypotheses have been proposed, the etiology of venous aneurysms remains unknown. Venous aneurysms are uncommon vascular malformations that affect both sexes equally and can occur at any age; they can appear as either a painful or painless subcutaneous mass. Upper extremity venous aneurysms have not been associated with any significant complications. For the most part, surgical excision is the only option. The patient, in this case, had a painless and mobile, soft, subcutaneous mass that was just a cosmetic issue.
It’s important to study other superficial veins of the upper limb to correlate them and understand the anatomy and pathology of the cephalic vein well.
Superficial Veins of the Upper Limb
Upper limb superficial veins are important in medical practice because they are widely used for intravenous injections and blood withdrawal for research.
Important Points
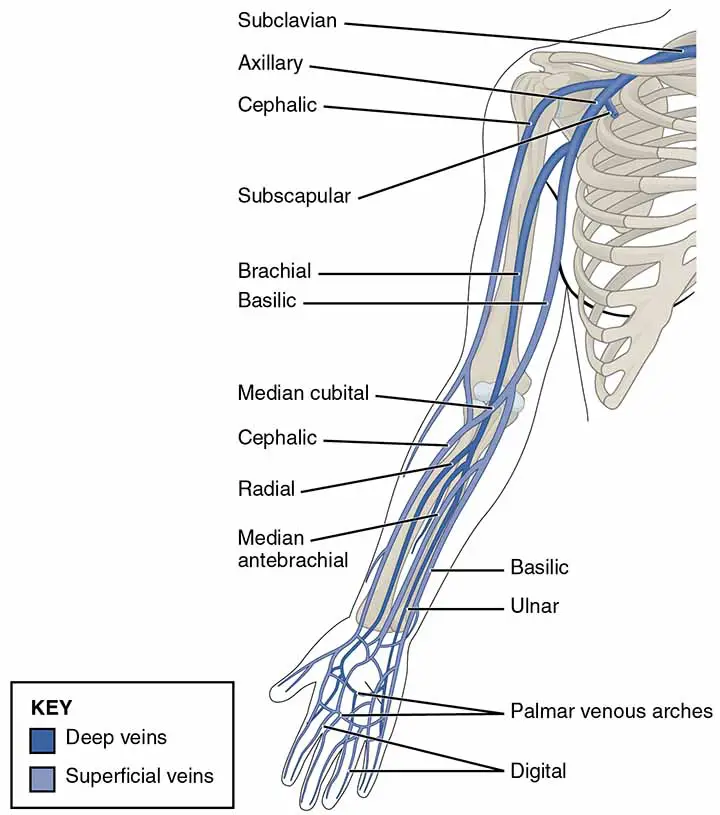
- The majority of the limb’s superficial veins connect to form two broad veins, the cephalic (preaxial) and basilic veins (postaxial). An accessory cephalic vein is often present.
- The superficial veins are those that run away from pressure points. As a result, they are missing from the palm (fist area), the ulnar border of the forearm (supporting border), and the back of the arm and trapezius region (resting surface). This causes the veins to spiral from the dorsal to the ventral surface of the limb.
- The preaxial vein is greater in length than the postaxial vein. In other words, the preaxial vein drains more proximally (at the root of the limb) into the deep (axillary) vein than the postaxial vein, which becomes deep in the middle of the arm.
- The sooner a vein becomes deep, the better since muscular compression aids venous return. The load of the preaxial (cephalic) vein is greatly relieved by the more powerful postaxial (basilic) vein via a short-circuiting channel (the median cubital vein located in front of the elbow) and, to a lesser extent, by the deep veins via a perforator vein linking the median cubital and the deep vein.
- Instead of arteries, superficial veins are surrounded by cutaneous nerves and superficial lymphatics. The superficial lymph nodes are located along the nerves, while the deep lymph nodes are located along the arteries.
- For intravenous injections, the superficial veins are particularly useful.
Dorsal Venous Arch
The dorsal venous arch is found on the hand. Its tributaries include;
- Three(3) dorsal metacarpal veins.
- A dorsal digital vein from the medial(ulnar side) side of the little finger.
- A dorsal digital vein from the radial(lateral) side of the index finger.
- Two dorsal digital veins from the thumb.
- The majority of the blood from the palm travels through veins that run along the hand’s margins, as well as perforating veins that run through the interosseous spaces. Due to the mode of drainage of the palm into the dorsal venous arch, pressure on the palm during gripping does not obstruct venous return. The cephalic and basilic veins are its efferents.
Read The Axillary Vein
Few Last Words
The cephalic vein is the preaxial vein of the arm. The median cubital vein connects it with the basilic vein. The median cubital vein is the most used vein for injection.
Last Updated on February 23, 2022 by Learn From Doctor Team




