Table of Contents
Pneumothorax X-ray Overview
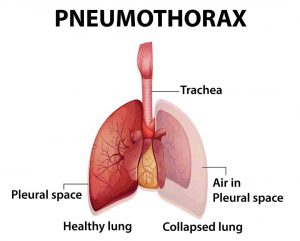
Pneumothorax x-ray (an upright posteroanterior chest x-ray) is essential to reach the provisional diagnosis of pneumothorax. The word “pneumothorax” (plural: pneumothoraces) means the presence of gas (usually air) in the pleural space. A tension pneumothorax occurs when a collection of gas continually expands, compressing mediastinal components and presenting a life-threatening danger (if no tension is present it is a simple pneumothorax). The term “occult pneumothorax” refers to a pneumothorax that was missed on initial imaging, which is typically a supine/semierect chest radiograph.
To read the case study of pneumothorax x-ray, follow the table of content or just read the end of this article.
Epidemiology of Pneumothorax
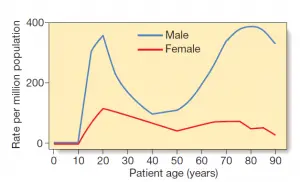
Since there are so many different causes of pneumothorax, it’s hard to generalize the epidemiology.
Primary spontaneous pneumothoraces occur in patients under the age of 35, on the other hand, secondary spontaneous pneumothoraces occur in patients over the age of 45 years.
Clinical Manifestations
The symptoms can vary from mild dyspnea to serious dyspnea with tachycardia and hypotension. Patients with a stress pneumothorax can present with distended neck veins and tracheal divergence, as well as cardiac arrest and, in the worst-case scenario, death.
It’s important to remember that some generalizations about its clinical appearance of primary and secondary spontaneous pneumothoraces can be made:
- Primary spontaneous: pleuritic chest pain is common, with mild to severe dyspnea.
- Secondary spontaneous: pleuritic chest pain is rarely present, and dyspnea is typically severe.
Some generalized symptoms for better understanding;
- Continuous chest pain
- Dyspnea(shortness of breath/breathlessness)
- Covered by cold sweat
- Feeling tightness around the chest
- Cyanosis(check 5 spots)
- Tachycardia
Causes of Pneumothorax
Generalized
- Primary spontaneous: No history of lung disease
- Secondary spontaneous: History of lung disease
- Traumatic
Primary Spontaneous Pneumothorax
The word “primary spontaneous pneumothorax” refers to a pneumothorax that arises in a patient who has no history of any lung disease. A primary spontaneous pneumothorax is more common in tall and thin people. There could be some genetic factors, and there are well-established links;
- Marfan syndrome
- Ehlers-Danlos syndrome
- alpha-1-antitrypsin deficiency
- homocystinuria
Secondary Spontaneous Pneumothorax
A secondary spontaneous pneumothorax occurs when there is the presence of some lung disease or abnormalities. Pneumothorax is caused by a variety of pulmonary diseases, including:
Parenchymal necrosis
- Lung abscess, fungal disease, TB, Necrotic type of pneumonia
- Cavitating neoplasm, metastatic osteogenic sarcoma
- Necrosis(Radiation)
- Pulmonary infarction may also responsible
Cystic lung diseases;
- Bulle
- Pulmonary emphysema
- Asthma
- PJP-Pneumocystis Jiroveci Pneumonia
- Honeycombing-Interstitial Lung Disease
- Lam-Lymphangiomyomatosis
- LCH-Langerhans Cell Histiocytosis
- Ankylosing Spondylitis
- Cystic fibrosis
Others
- Catamenial pneumothorax: chronic spontaneous pneumothorax associated with pleural endometriosis throughout menstruation.
- Pleuroparenchymal fibroelastosis(PPFE) is a very rare condition.
Traumatic Pneumothorax
- Laceration(pulmonary)
- Rupture(bronchotrachial)
- acupuncture
- Rupture of the Oesophagus
Iatrogenic
- percutaneous biopsy
- barotrauma & ventilators
- radiotherapy (Radiofrequency)
- Perforation of Oesophagus due to endoscopy
- Nasogastric tube
Associated causes
- pneumoperitoneum with passage through pathological diaphragmatic defects
- buffalo pneumothorax
Read Tension Pneumothorax
Risk Factors of Pneumothorax
Risk Factors of Spontaneous Pneumothorax
- Younger people
- Thin body built
- Male
- 10-30 year old
- Congenital lung diseases
- Smokers
Those who are having lung disease and age are over 40 are the most at risk.
Risk Factors of Traumatic Pneumothorax
- Physical sports such as; football, rugby
- Performing dangerous stunts
- Fighting
- Road traffic accidents
- Fall from height
- Recent medical conditions of the lung
Diagnosis of Pneumothorax
The presence of gas in the area around the lungs is used to make a diagnosis. A stethoscope can reliably detect lung vibrations, but it can be difficult to identify a small pneumothorax. Because of the air between the chest wall and the lung, certain imaging tests can be difficult to interpret.
- Pneumothorax chest x-ray
- Ct Scan
- Thoracic Ultrasound
Pneumothorax Chest x-ray features
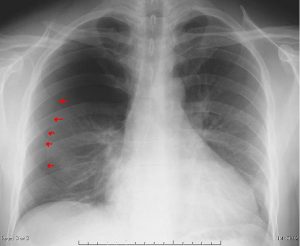
Plain x-ray(radiograph)
When looking for a pneumothorax, upright chest radiographs are normally helpful.
- A very thin, sharp white line is noticeable as the visceral pleural edge.
- There are no lung marks on this line’s periphery.
- In contrast to the adjacent lung, the peripheral space is radiolucent.
- It’s possible that the lung could absolutely collapse.
- If a stress pneumothorax is present, the mediastinum does not move away from the pneumothorax
- There may also be subcutaneous emphysema including pneumomediastinum.
The following are some of the methods for estimating the percentage volume of pneumothorax from an erect Posteroanterior radiograph that has been mentioned.
Method of Collins
- The percentage (%) of pneumothorax = 4.7 (A + B + C) + 4.2
- The maximum apical interpleural distance is denoted by the letter A.
- B is the interpleural gap in the upper half of the lung at its midpoint.
- C is the interpleural gap at the lower half of the lung’s midpoint.
Light Index Method
- The percentage(%) of pneumothorax = 100−(DL3/DH3×100)
- DLis the collapsed lung’s diameter.
- DHis the collapsed side of the hemithorax’s diameter.
Method of RHEA
A variety of techniques can be used when a pneumothorax is not plainly apparent on standard posteroanterior chest radiography;
X-ray at lateral decubitus
The lung can ‘roll’ away from the chest wall if performed with the expected side up.
Expiratory chest x-ray
Even though some authors claim that there is no change in detection rate, the pneumothorax stays the same scale and therefore is more noticeable.
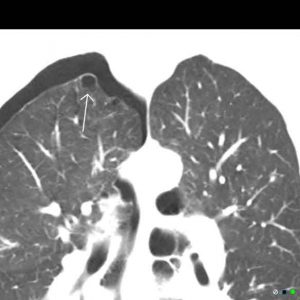
CT Scan
A pneumothorax can be easily detected on CT if the lung openings are checked, and it should pose little diagnostic difficulty. A loculated pneumothorax can mimic a bullous pneumothorax when bullous disease is present.
Pneumothorax Ultrasound
The M-mode can be used to assess lung activity in the rib-interspace. Small pneumothoraces are best seen anteriorly (gas rises) in the supine position, while broad pneumothoraces are best seen laterally in the mid-axillary rows.
Treatment of Pneumothorax
Treatment of pneumothorax depends on some factors, such as;
- Pneumothorax size and shape
- History of lung diseases
- Symptoms of pneumothorax
There is no international agreement on how to measure the size of a pneumothorax. CT scans are thought to be more precise than traditional radiographs.
According to British Thoracic Society: Measured at the level of the hilum from the chest wall to the lung edge.
- Smaller than 2 cm = Small
- Greater than or equal to 2 cm = Large
According to the American College of Chest Physician: The distance between the thoracic cupola and the apex of the lung.
- Smaller than 3 cm = Small
- Greater than or equal to 3 cm = Large
The treatment of Pneumothorax according to the British Thoracic Society
- A small rim of pneumothorax which is asymptomatic: No treatment, suggested follow-up x-ray to ensure resolution.
- Pneumothorax with mild nonspecific or specific symptoms(without any underlying lung disease): Aspiration of the needle in the first instance.
- Pneumothorax with significant symptoms and chronic underlying lung diseases or conditions: Intercostal drain insertion following Seldinger Technique.
Pleurodesis is a treatment that may be performed on patients that have recurrent pneumothoraces or who are at a very high risk of having recurrent incidents and have a low respiratory capacity. This may be medical (for example, talc poudrage) or surgical (e.g. VATS pleurectomy, pleural abrasion, sclerosing agent).
Pneumothorax Recovery: For patients
The recovery time from a pneumothorax is usually 1 to 2 weeks.
- Return to your normal routine gradually. Take walks or participate in other low-impact sports.
- Keep an eye on your symptoms. Keep an eye out for chest pains or other indications that you haven’t fully recovered, such as a fever or blood in your coughing.
- Only light items should be lifted. Anything heavier than a gallon of milk should be avoided. Vacuuming and mowing the lawn are not recommended.
- Be cautious about how you workout. Do not participate in any behaviors that cause the body to jar, such as hiking or biking. Playing contact sports is not a good idea.
- Bear in mind the importance of atmospheric pressure. Do not board a plane until your doctor gives you the go-ahead, which is normally 3 weeks after your lungs has been fixed. Don’t go higher than 7,500 feet above sea level on land.
Differential Diagnosis of Pneumothorax
- Artifacts: Gas(air) caught between chest outside structures
- Skinfold: As contrasted to a genuine pneumothorax, which is a white pleural edge, the apparent pleural edge is denser (i.e. black). It may stretch beyond the chest cavity or fade out.
- Clothing
- Blankets
- Oxygen Bags
- The overlapping margin of the breast
- Normal anatomical structures
- Bullae(Pulmonary)
- Giant bullous emphysema
- Pseudopneumoperitoneum(Post traumatic-not chronic)
- Pleural plucks
- Pneumomediastinum
- Pneumopericardium
- Hemithorax(Hyperlucent)
- In CT Scan:
- Air in Brachiocephalic vein due to cannulation
- Beam hardening artifacts







Prevention Strategy of Pneumothorax
- If you smoke, speak with your doctor about stopping.
- Your doctor may advise you to stop scuba diving.
- Keep up with your doctor appointments if you have a lung infection.
Pneumothorax X-ray Case Study
























Few Last Words
Pneumothorax diagnosis depends on how perfectly a doctor reads a pneumothorax x-ray film. Hope, you can enrich your knowledge with all of those case studies and discussion.
Last Updated on February 23, 2022 by Learn From Doctor Team




